

Lymphatic System. In anatomy, the lymphatic system (Lat. lympha, clear water) comprises the lymphoid or adenoid tissue so plentifully distributed about the body, especially in the course of the alimentary canal (see Connective Tissues), lymph spaces, lymphatic vessels of which the lacteals are modifications, lymphatic glands, haemolymph glands, and the thoracic and right lymphatic ducts by which the lymph (q.v.) finally reaches the veins.
Lymph spaces are mere spaces in the connective tissue, which usually have no special lining, though sometimes there is a layer of endothelial cells like those of the lymphatic and blood vessels. Most of these spaces are very small, but sometimes, as in the case of the sub-epicranial space of the scalp, the capsule of Tenon in the orbit, and the retropharyngeal space in the neck, they are large and are adaptations to allow free movement. Opening from these spaces, and also communicating with the serous membranes by small openings called stomata,1 are the lymph capillaries (see Vascular System), which converge to the lymphatic vessels. These resemble veins in having an internal layer of endothelium, a middle unstriped muscular coat, and an external coat of fibrous tissue, though in the smaller vessels the middle coat is wanting. They have numerous endothelial valves, formed of two crescentic segments allowing the lymph to pass toward the root of the neck. When the vessels are engorged these valves are marked by a constriction, and so the lymphatics have a beaded appearance. The vessels divide and anastomose very freely, and for this reason they do not, like the veins, increase in calibre as they approach their destination. It is usual to divide the lymphatic vessels into a superficial and a deep set; speaking generally, the superficial ones are found near the course of the superficial veins, while the deeper ones accompany the arteries. Probably any single drop of lymph passes sooner or later through one or more lymphatic glands, and so those vessels which are approaching a gland are called afferent, while those leaving are spoken of as efferent lymphatics. The lacteals are special lymphatic vessels which carry the chyle from the intestine; they begin in lymphatic spaces in the villi and round the solitary and agminated glands, and pass into the mesentery, where they come in contact with a large number of mesenteric glands before reaching the receptaculum chyli.
The lymphatic glands are pink bodies situated in the course of the lymphatic vessels, to which they act as filters. They are generally oval in shape and about the size of a bean, but sometimes, especially in the groin, they form irregular flattened masses 2 in. long, while, at other times, they are so small as almost to escape notice. They are usually found in groups.
Each gland has a fibrous capsule from which trabeculae pass toward the centre, where they break up and interlace, forming a network, and in this way a cortical and medullary region for each gland is distinguished; the intervals are nearly filled by lymphoid tissue, but close to the trabeculae is a lymph path or sinus, which is only crossed by the reticular stroma of the lymphoid tissue, and this probably acts as a mechanical sieve, entangling foreign particles; as an example of this the bronchial glands are black from carbon strained off in its passage from the lungs, while the axillary glands in a tattooed arm are blue. The blood-vessels enter at one spot, the hilum, and are distributed along the trabeculae. In addition to their function as filters the lymphatic glands are probably one of the sources from which the leucocytes are derived.
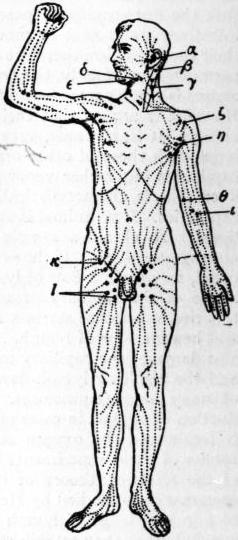 |
| Fig. 1.—Superficial Lymphatic Vessels and Glands. |
α, Preauricular. β, Mastoid. γ, Superficial cervical. δ, Submaxillary. ε, Submental. ζ, Infraclavicular. η, Anterior axillary. θ, Supratrochlear. ι, Antecubital. κ, Inguinal. λ, Superficial femoral. |
The exact position of the various groups of glands is very important from a medical point of view, but here it is only possible to give a brief sketch which will be helped by reference to the accompanying diagram. In the head are found occipital and mastoid glands (fig. 1, β), which drain the back of the scalp; internal maxillary glands, in the zygomatic fossa, draining the orbit, palate, nose and membranes of the brain; preauricular glands (fig. 1, α), embedded in the parotid, draining the side of the scalp, pinna, tympanum and lower eyelid; and buccal glands, draining the cheek region. In the neck are the superficial cervical glands (fig. 1, γ), along the course of the external jugular vein, draining the surface of the neck; the submaxillary glands (fig. 1, δ), lying just above the salivary gland of the same name and draining the front of the face and scalp; the submental glands (fig. 1, ε), beneath the chin, draining the lower lip, as well as sometimes the upper, and the front of the tongue; the retropharyngeal glands, draining the naso-pharynx and tympanum; the pretracheal glands, draining the trachea and lower part of the thyroid body; and the deep cervical glands, which are by far the most important and form a great mass close to the internal jugular vein; they receive afferent vessels from most of the glands already mentioned and so are liable to be affected in any trouble of the head or neck, especially of the deeper parts. Into them the lymphatics of the brain pass directly. The lower part of this mass is sometimes distinguished as a separate group called the supra-clavicular glands, which drain the back of the neck and receive afferents from the occipital and axillary glands. The efferents from the deep cervical glands join to form a common vessel known as the jugular lymphatic trunk, and this usually opens into the thoracic duct on the left side and the right lymphatic duct on the right.
In the thorax are found intercostal glands (fig. 2, I.), near the vertebral column draining the back of the thoracic walls and pleura; internal mammary glands, draining the front of the same parts as well as the inner part of the breast and the upper part of the abdominal wall; diaphragmatic glands, draining that structure and the convex surface of the liver; anterior, middle, posterior and superior mediastinal glands, draining the contents of those cavities. The bronchial glands, draining the lungs, have already been referred to.
In the abdomen and pelvis the glands are usually grouped round the large arteries and are divided into visceral and parietal. Among the visceral are the gastric glands, draining the stomach (these are divided into coronary, subpyloric and retropyloric groups); the splenic glands at the hilum of the spleen, draining that organ, the tail of the pancreas and the fundus of the stomach; the hepatic glands in the small omentum, draining the lower surface and deep parts of the liver; the pancreatic glands, behind the lesser sac of the peritoneum, draining the head and body of the pancreas, the superior mesenteric glands; from one to two hundred in number, lying in the mesentery and receiving the lacteals; the ileo-caecal glands, draining the caecum, one of which is known as the appendicular gland and drains the vermiform appendix and right ovary; the colic glands along the right and middle colic arteries, draining the ascending and transverse colon; the inferior mesenteric glands in the course of that artery, draining the descending iliac and pelvic colons; the rectal glands, behind the rectum, draining its upper part.
Among the parietal glands are the external iliac glands, divided into a lateral and mesial set (see fig. 2, E.I.), and receiving the inguinal efferent vessels and lymphatics from the bladder, prostate, cervix uteri, upper part of the vagina, glans penis vel clitoridis and urethra. The supra and infra-umbilical glands receive the deep lymphatics of the abdominal wall, the former communicating with the liver, the latter with the bladder. From the latter, vessels pass to the epigastric gland lying in front of the termination of the external iliac artery. The internal iliac glands (fig. 2, I. I.) are situated close to the branches of this artery and drain the rectum, vagina, prostate, urethra, buttock and perinaeum. Common iliac glands (fig. 2, C.I.) lie around that artery and receive afferents from the external and internal iliac glands as well as a few from the pelvic viscera.2 The aortic glands are grouped all round the length of the aorta, and are divided into pre-, retro- and lateral aortic groups (fig. 2 P.A. and L), all of which communicate freely. The upper preaortic glands are massed round the coeliac axis, and receive afferents from the gastric, hepatic, splenic and pancreatic glands; they are known as coeliac glands. The lateral aortic glands drain the kidney, adrenal, testis, ovary, fundus of uterus and lateral abdominal walls. In the upper extremity a few small glands are sometimes found near the deep arteries of the forearm. At the bend of the elbow are the ante-cubital glands (fig. 1 λ) and just above the internal condyle, one or two supra-trochlear glands (fig. 1, θ). The axillary glands (fig. 1, η) are perhaps the most practically important in the body. They are divided into four sets: (1) external, along the axillary vessels, draining the greater part of the arm; (2) anterior, behind the lower border of the pectoralis major muscle, draining the surface of the thorax including the breast and upper part of the abdomen; (3) posterior along the subscapular artery, draining the back and side of the trunk as low as the umbilical zone; (4) superior or infra-clavicular glands (fig. 1, ζ), receiving the efferents of the former groups as well as lymphatics accompanying the cephalic vein. In the lower limb all the superficial lymphatics pass up to the groin, where there are two sets of glands arranged like a T. The superficial femoral glands (fig. 1, λ) are the vertical ones, and are grouped round the internal saphenous vein; they are very large, drain the surface of the leg, and are usually in two parallel rows. The inguinal glands form the cross bar of the T (fig. 1, κ), and drain part of the buttock, the surface of the abdomen below the umbilicus and the surface of the genital organs. The deep lymphatics of the leg drain into the anterior tibial gland on that artery, the popliteal glands in that space, and the deep femoral glands surrounding the common femoral vein.
 |
|
| From A. M. Paterson, Cunningham’s Text-book of Anatomy. | |
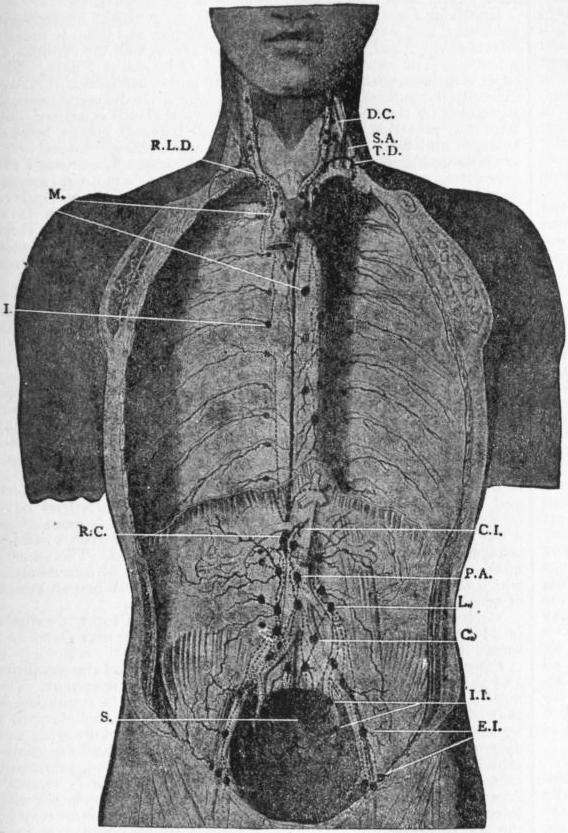
| Fig. 2.—Deep Lymphatic Glands and Vessels of the Thorax and Abdomen (diagrammatic). Afferent vessels are represented by continuous lines and efferent and interglandular vessels by dotted lines. | |
C. Common iliac glands. C.I. Common intestinal trunk. D.C. Deep cervical glands. E.I. External iliac glands. I. Intercostal glands and vessels. I.I. Internal iliac glands. L. Lateral aortic glands. |
M. Mediastinal glands and vessels. P.A. Pre-aortic glands and vessels. R.C. Receptaculum chylii. R.L.D. Right lymphatic duct. S. Sacral glands. S.A. Scalenus anticus muscle. T.D. Thoracic duct. |
The thoracic duct begins as an irregular dilatation known as the receptaculum chyli, opposite the first and second lumbar vertebrae, which receives all the abdominal lymphatics as well as those of the lower intercostal spaces. The duct runs up on the right of the aorta through the posterior mediastinum and then traverses the superior mediastinum to the left of the oesophagus. At the root of the neck it receives the lymphatics of the left arm and left side of the neck and opens into the beginning of the left innominate vein, usually by more than one opening.
The right lymphatic duct collects the lymphatics from the right side of the neck and thorax, the right arm, right lung, right side of the heart and upper surface of the liver; it is often represented by several ducts which open separately into the right innominate vein.
Haemolymph glands are structures which have only been noticed since 1884. They differ from lymphatic glands in their much greater vascularity. They assist the spleen in the destruction of red blood corpuscles, and probably explain or help to explain the fact that the spleen can be removed without ill effects. In man they extend along the vertebral column from the coeliac axis to the pelvis, but are specially numerous close to the renal arteries.
T. Lewis suggests that lymphatic and haemolymph glands should be classified in the following way:—
| Haemolymph Glands. | Haemal glands. | Simple. |
| Specialized (Spleen) | ||
| Haemal lymphatic glands. | 1. Blood and lymph sinuses separate. | |
| 2. Blood lymph sinuses. | ||
| 3. Other combined forms. | ||
| Lymphatic glands. |
Details and references will be found in papers by T. Lewis, J. Anat. & Phys. vol. xxxviii. p. 312; W. B. Drummond, Journ. Anat. and Phys. vol. xxxiv. p. 198; A. S. Warthin, Journ. Med. Research, 1901, p. 3, and H. Dayton, Am. Journ. of Med. Sciences, 1904, p. 448. For further details of man’s lymphatic system see The Lymphatics by Delamere, Poirier and Cuneo, translated by C. H. Leaf (London, 1903).
Embryology.—The lymphatic vessels are possibly developed by the hollowing out of mesenchyme cells in the same way that the arteries are; these cells subsequently coalesce and form tubes (see Vascular System). There is, however, a good deal of evidence to show that they are originally offshoots of the venous system, and that their permanent openings into the veins are either their primary points of communication or are secondarily acquired. The lymphatic and haemolymph glands are probably formed by the proliferation of lymphocytes around networks of lymphatic vessels; the dividing lymphocytes form the lymphoid tissue, and eventually the network breaks up to form distinct glands into which blood vessels penetrate. If the blood vessels enlarge more than the lymphatic, haemolymph glands result, but if the lymphatic vessels become predominant ordinary lymphatic glands are formed. At an early stage in the embryo pig two thoracic ducts are formed, one on either side of the aorta, and the incomplete fusion of these may account for the division often found in man’s duct. In the embryo pig too there have been found two pairs of lymph hearts for a short period.
See A. S. Warthin, Journ. Med. Research, vol. vii. p. 435; F. R. Sabin, Am. Journ. of Anat. i., 1902; and, for literature, Development of the Human Body, by J. P. McMurrich (London, 1906), and Quain’s Anatomy (vol. i., London, 1908).
Comparative Anatomy.—A lymphatic system is recognized in all the Craniata, and in the lower forms (fishes and Amphibia) it consists chiefly of lymph spaces and sinuses in communication with the coelom. In fishes, for instance, there is a large subvertebral lymph sinus surrounding the aorta and another within the spinal canal. In Amphibia the subvertebral sinus is also found, and in the Anura (frogs and toads) there is a great subcutaneous lymph sinus. Lymph hearts are muscular dilatations of vessels and are found in fishes, amphibians, reptiles and bird embryos, and drive the lymph into the veins; they are not known in adult mammals.
In birds the thoracic duct is first recognized, and opens into both right and left precaval veins, as it always does in some mammals. In birds, however, some of the lymphatics open into the sacral veins, and it is doubtful whether true lymphatic glands ever occur. In birds and mammals lymphatic vessels become more definite and numerous and are provided with valves.
Haemolymph glands are present in mammals and birds, but have not been seen lower in the scale, though S. Vincent and S. Harrison point out the resemblance of the structure of the head kidney of certain Teleostean fishes to them (Journ. Anat. and Phys. vol. xxxi. p. 176).
For further details see Comparative Anat. of Vertebrates, by R. Wiedersheim (London, 1907).
Diseases of the Lymphatic System and Ductless Glands.
Lymphadenitis or inflammatory infection of the lymphatic glands, is a condition characterized by hyperaemia of and exudation into the gland, which becomes reader, firmer and larger than usual. Three varieties may be distinguished: simple, suppurative and tuberculous. The cause is always the absorption of some toxic or infective material from the periphery. This may take place in several of the acute infectious diseases, notably in scarlet fever, mumps, diphtheria and German measles, or may be the result of poisoned wounds. The lymphatic glands are also affected in constitutional diseases such as syphilis. Simple lymphadenitis usually subsides of its own accord, but if toxins are produced in the inflamed area the enlargement is obvious and painful, while if pyogenic organisms are absorbed the inflammation progresses to suppuration.
Tuberculous lymphadenitis (scrofula) is due to the infection of the lymph glands by Koch’s tubercle bacillus. This was formerly known as “King’s Evil,” as it was believed that the touch of the royal hand had power to cure it. It occurs most commonly in children and young adults whose surroundings are unhealthy, and who are liable to develop tuberculous disease from want of sufficient food and fresh air. Some local focus of irritation is usually present. The ways in which the tubercle bacillus enters the body are much disputed, but catarrh of the mucous membranes is regarded as a predisposing factor, and the tonsils as a probable channel of infection. Any lymphoid tissue in the body may be the seat of tuberculous disease, but the glands of the neck are the most commonly involved. The course of the disease is slow and may extend over a period of years. The earliest manifestation is an enlargement of the gland. It is possible in this stage for spontaneous healing to take place, but usually the disease progresses to caseation, in which tuberculous nodules are found diffused throughout the gland. Occasionally this stage may end in calcification of the caseous matter, the gland shrinking and becoming hard; but frequently suppuration follows from liquefaction of the caseating material. Foci of pus occur throughout the gland, causing destruction of the tissue, so that the gland may become a single abscess cavity. If left to itself the abscess sooner or later bursts at one or several points, leaving ulcerated openings through which a variable amount of pus escapes. Temporary healing may take place, to be again followed by further breaking down of the gland. This condition, if untreated, may persist for years and may finally give rise to a general tuberculosis. The treatment consists mainly in improving the general health with good diet, fresh air (particularly sea air), cod-liver oil and iron, and the removal of all sources of local irritation such as enlarged tonsils, adenoids, &c. Vaccination with tuberculin (TR) may be useful. Suppuration and extension of the disease require operative measures, and removal of the glands en masse can now be done through so small an opening as to leave only a very slight scar.
In Tabes mesenterica (tuberculosis of the mesenteric glands), usually occurring in children, the glands of the mesentery and retroperitonaeum become enlarged, and either caseate or occasionally suppurate. The disease may be primary or may be secondary to tuberculous disease of the intestines or to pulmonary phthisis. The patients are pale, wasted and anaemic, and the abdomen may be enormously enlarged. There is usually moderate fever, and thin watery diarrhoea. The caseating glands may liquefy and give rise to an inflammatory attack which may simulate appendicitis. Limited masses are amenable to surgical treatment and may be removed, while in the earlier stages constitutional treatment gives good results. Tuberculous peritonitis frequently supervenes on this condition.
Lymphadenoma (Hodgkin’s Disease), a disease which was first fully described by Hodgkin in 1832, is characterized by a progressive enlargement of the lymphatic glands all over the body, and generally starts in the glands of the neck. The majority of cases occur in young adults, and preponderate in the male sex. The first symptom is usually enlargement of a gland in the neck, with generally progressive growth of the glands in the submaxillary region and axilla. The inguinal glands are early involved, and after a time the internal lymph glands follow. The enlargements are at first painless, but in the later stages symptoms are caused by pressure on the surrounding organs, and when the disease starts in the deeper structures the first symptoms may be pain in the chest and cough, pain in the abdomen, pain and oedema in the legs. The glands may increase until they are as large as eggs, and later may become firmly adherent one to another, forming large lobulated tumours. Increase of growth in this manner in the neck may cause obstructive dyspnoea and even death. In the majority of cases the spleen enlarges, and in rare instances lymphoid tumours may be found on its surface. Anaemia is common and is secondary in character; slight irregular fever is present, and soon a great and progressive emaciation takes place. The cases are of two types, the acute cases in which the enlargements take place rapidly and death may occur in two to three months, and the chronic cases in which the disease may remain apparently stationary. In acute lymphadenoma the prognosis is very unfavourable. Recovery sometimes takes place in the chronic type of the disease. Early surgical intervention has in some cases been followed by success. The application of X-rays is a valuable method of treatment, superficial glands undergoing a rapid diminution in size. Of drugs arsenic is of the most service, and mercurial inunction has been recommended by Dreschfeld. Organic extracts have of late been used in the treatment of lymphadenoma.
Glandular Fever is an acute infectious fever, generally occurring in epidemics, and was first described by E. Pfeiffer in 1889. It usually affects children and has a tendency to run through all the children of a family. The incubation period is said to be about 7 days. The onset is sudden, with pain in the neck and limbs, headache, vomiting, difficulty in swallowing and high temperature. On the second day, or sometimes on the first, swelling of the cervical glands is noticed, and later the posterior cervical, axillary and inguinal glands become enlarged and tender. In about half the cases the spleen and liver are enlarged and there is abdominal tenderness. West found the mesenteric nodes enlarged in 37 cases. Nephritis is an occasional complication, and constipation is very usual. The disease tends to subside of itself, and the fever usually disappears after a few days; the glandular swellings may, however, persist from one to three weeks. Considerable anaemia has been noticed to follow the illness. Rest in bed while the glands are enlarged, and cod-liver oil and iron to meet the anaemia, are the usual treatment.
Status lymphaticus (lymphatism) is a condition found in children and some adults, characterized by an enlargement of the lymphoid tissues throughout the body and more particularly by enlargement of the thymus gland. There is a special lowering of the patient’s powers of resistance, and it has been said to account for a number of cases of sudden death. In all cases of status lymphaticus the thymus has been found enlarged. At birth the gland (according to Bovaird and Nicoll) weighs about 6 grammes, and does not increase after birth. In lymphatism it may weigh from 10 to 50 grammes. The clinical features are indefinite, and the condition frequently passes unrecognized during life. In most cases there is no hint of danger until the fatal syncope sets in, which may be after any slight exertion or shock, the patient becoming suddenly faint, gasping and cyanosed, and the heart stopping altogether before the respirations have ceased. The most trifling causes have brought on fatal issues, such as a wet pack (Escherich) or a hypodermic injection, or even a sudden plunge into water though the head is not immersed. The greater number of deaths occur during the administration of anaesthetics, which seem peculiarly dangerous to these subjects. When an attack of syncope takes place no treatment is of any avail.
Virchow, West and Goodhardt have described a form of asthma in adults which they ascribe to a hypertrophied thymus gland and term “thymic asthma.”
Diseases of the Spleen.—Physiological variations and abnormalities and absence of the spleen are so rare as to require no comment. The most usual pathological condition which gives rise to symptoms is that of wandering spleen, which may or may not be secondary to a wandering left kidney. It may produce symptoms of dragging and discomfort, dyspepsia, vomiting and abdominal pain, and sometimes jaundice (Treves), or the pedicle may become twisted, producing extremely severe symptoms. The treatment is entirely surgical. Abscess in the spleen occasionally occurs, usually in association with infective endocarditis or with general pyaemia. The spleen may be the seat of primary new growths, but these are rare, and only in a small portion of cases does it share in the metastatic reproduction of carcinoma. Infection of the spleen plays a prominent part in many diseases, such as malaria, typhoid fever, lymphadenoma and leucaemia.
Diseases of the thyroid gland (see Goitre) and Addison’s disease (of the suprarenal glands) are treated separately.