

Eye (O. Eng. eáge, Ger. Auge); derived from an Indo-European root also seen in Lat. oc-ulus, the organ of vision (q.v.).
Anatomy.—The eye consists of the eyeball, which is the true organ of sight, as well as of certain muscles which move it, and of the lachrymal apparatus which keeps the front of it in a moist condition. The eyeball is contained in the front of the orbit and is a sphere of about an inch (24 mm.) in diameter. From the front of this a segment of a lesser sphere projects slightly and forms the cornea (fig. 1, co). There are three coats to the eyeball, an external (protective), a middle (vascular), and an internal (sensory). There are also three refracting media, the aqueous humour, the lens and the vitreous humour or body.
 |
|
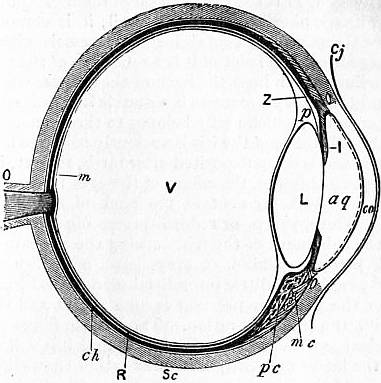
| Fig. 1.—Diagrammatic Section through the Eyeball. | |
cj, Conjunctiva. co, Cornea. Sc, Sclerotic. ch, Choroid. pc, Ciliary processes. mc, Ciliary muscle. O, Optic nerve. R, Retina. I, Iris. |
aq, Anterior chamber of aqueous humour. L, Lens. V, Vitreous body. Z, Zonule of Zinn, the ciliary process being removed to show it. p, Canal of Petit. m, Yellow spot. The dotted line behind the cornea represents its posterior epithelium. |
The protective coat consists of the sclerotic in the posterior five-sixths and the cornea in the anterior sixth. The sclerotic (fig. 1, Sc) is a firm fibrous coat, forming the “white of the eye,” which posteriorly is pierced by the optic nerve and blends with the sheath of that nerve, while anteriorly it is continued into the cornea at the corneo-scleral junction. At this point a small canal, known as the canal of Schlemm, runs round the margin of the cornea in the substance of the sclerotic (see fig. 1). Between the sclerotic and the subjacent choroid coat is a lymph space traversed by some loose pigmented connective tissue,—the lamina fusca. The cornea is quite continuous with the sclerotic but has a greater convexity. Under the microscope it is seen to consist of five layers. Most anteriorly there is a layer of stratified epithelium, then an anterior elastic layer, then the substantia propria of the cornea which is fibrous with spaces in which the stellate corneal corpuscles lie, while behind this is the posterior elastic layer and then a delicate layer of endothelium. The transparency of the cornea is due to the fact that all these structures have the same refractive index.
The middle or vascular coat of the eye consists of the choroid, the ciliary processes and the iris. The choroid (fig. 1, ch) does not come quite as far forward as the corneo-scleral junction: it is composed of numerous blood-vessels and pigment cells bound together by connective tissue and, superficially, is lined by a delicate layer of pigmented connective tissue called the lamina suprachoroidea in contact with the already-mentioned perichoroidal lymph space. On the deep surface of the choroid is a structureless basal lamina.
The ciliary processes are some seventy triangular ridges, radially arranged, with their apices pointing backward (fig. 1, pc), while their bases are level with the corneo-scleral junction. They are as vascular as the rest of the choroid, and contain in their interior the ciliary muscle, which consists of radiating and circular fibres. The radiating fibres (fig. 1, mc) rise, close to the canal of Schlemm, from the margin of the posterior elastic lamina of the cornea, and pass backward and outward into the ciliary processes and anterior part of the choroid, which they pull forward when they contract. The circular fibres lie just internal to these and are few or wanting in short-sighted people.
The iris (fig. 1, I) is the coloured diaphragm of the eye, the centre of which is pierced to form the pupil; it is composed of a connective tissue stroma containing blood-vessels, pigment cells and muscle fibres. In front of it is a reflection of the same layer of endothelium which lines the back of the cornea, while behind both it and the ciliary processes is a double layer of epithelium, deeply pigmented, which really belongs to the retina. The pigment in the substance of the iris is variously coloured in different individuals, and is often deposited after birth, so that, in newly-born European children, the colour of the eyes is often slate-blue owing to the black pigment at the back of the iris showing through. White, yellow or reddish-brown pigment is deposited later in the substance of the iris, causing the appearance, with the black pigment behind, of grey, hazel or brown eyes. In blue-eyed people very little interstitial pigment is formed, while in Albinos the posterior pigment is also absent and the blood vessels give the pink coloration. The muscle fibres of the iris are described as circular and radiating, though it is still uncertain whether the latter are really muscular rather than elastic. On to the front of the iris, at its margin, the posterior layer of the posterior elastic lamina is continued as a series of ridges called the ligamentum pectinatum iridis, while between these ridges are depressions known as the spaces of Fontana.
The inner or sensory layer of the wall of the eyeball is the retina; it is a delicate transparent membrane which becomes thinner as the front of the eye is approached. A short distance behind the ciliary processes the nervous part of it stops and forms a scalloped border called the ora serrata, but the pigmented layer is continued on behind the ciliary processes and iris, as has been mentioned, and is known as the pars ciliaris retinae and pars iridica retinae. Under the microscope the posterior part of the retina is seen to consist of eight layers. In its passage from the lens and vitreous the light reaches these layers in the following order:—(1) Layer of nerve fibres; (2) Layer of ganglion cells; (3) Inner molecular layer; (4) Inner nuclear layer; (5) Outer molecular layer; (6) Outer nuclear layer; (7) Layer of rods and cones; (8) Pigmented layer.
The layer of nerve fibres (fig. 2, 2) is composed of the axis-cylinders only of the fibres of the optic nerve which pierce the sclerotic, choroid and all the succeeding layers of the retina to radiate over its surface.
The ganglionic layer (fig. 2, 3) consists of a single stratum of large ganglion cells, each of which is continuous with a fibre of the preceding layer which forms its axon. Each also gives off a number of finer processes (dendrites) which arborize in the next layer.
The inner molecular layer (fig. 2, 4) is formed by the interlacement of the dendrites of the last layer with those of the cells of the inner nuclear layer which comes next.
The inner nuclear layer (fig. 2, 5) contains three different kinds of cells, but the most important and numerous are large bipolar cells, which send one process into the inner molecular layer, as has just been mentioned, and the other into the outer molecular layer, where they arborize with the ends of the rod and cone fibres.
The outer molecular layer (fig. 2, 6) is very narrow and is formed by the arborizations just described. The outer nuclear layer (fig. 2, 7), like the inner, consists of oval cells, which are of two kinds. The rod granules are transversely striped, and are connected externally with the rods, while internally processes pass into the outer molecular layer to end in a knob around which the arborizations of the inner nuclear cells lie. The cone granules are situated more externally, and are in close contact with the cones; internally their processes form a foot-plate in the outer molecular layer from which arborizations extend.
The layer of rods and cones (fig. 2, 9) contains these structures, the rods being more numerous than the cones. The rods are spindle-shaped bodies, of which the inner segment is thicker than the outer. The cones are thicker and shorter than the rods, and resemble Indian clubs, the handles of which are directed outward and are transversely striped. In the outer part of the rods the visual purple or rhodopsin is found.
The pigmented layer consists of a single layer of hexagonal cells containing pigment, which is capable of moving towards the rods and cones when the eye is exposed to light and away from them in the dark.
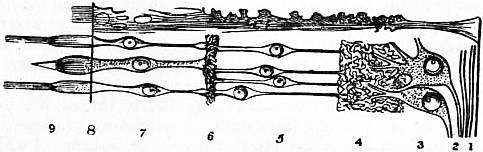 |
| Fig. 2.—Diagrammatic section through the retina to show the several layers, which are numbered as in the text. Ct, The radial fibres of the supporting connective tissue. |
Supporting the delicate nervous structures of the retina are a series of connective tissue rods known as the fibres of Müller (fig. 2, Ct); these run through the thickness of the retina at right angles to its surface, and are joined together on the inner side of the layer of nerve fibres to form the inner limiting membrane. More externally, at the bases of the rods and cones, they unite again to form the outer limiting membrane.
When the retina is looked at with the naked eye from in front two small marks are seen on it. One of these is an oval depression about 3 mm. across, which, owing to the presence of pigment, is of a yellow colour and is known as the yellow spot (macula lutea); it is situated directly in the antero-posterior axis of the eyeball, and at its margin the nerve fibre layer is thinned and the ganglionic layer thickened. At its centre, however, both these layers are wanting, and in the layer of rods and cones only the cones are present. This central part is called the fovea centralis and is the point of acutest vision. The second mark is situated a little below and to the inner side of the yellow spot; it is a circular disk with raised margins and a depressed centre and is called the optic disk; in structure it is a complete contrast to the yellow spot, for all the layers except that of the nerve fibres are wanting, and consequently, as light cannot be appreciated here, it is known as the “blind spot.” It marks the point of entry of the optic nerve, and at its centre the retinal artery appears and divides into branches. An appreciation of the condition of the optic disk is one of the chief objects of the ophthalmoscope.
The crystalline lens (fig. 1, L) with its ligament separates the aqueous from the vitreous chamber of the eye; it is a biconvex lens the posterior surface of which is more curved than the anterior. Radiating from the anterior and posterior poles are three faint lines forming a Y, the posterior Y being erect and the anterior inverted. Running from these figures are a series of lamellae, like the layers of an onion, each of which is made up of a number of fibrils called the lens fibres. On the anterior surface of the lens is a layer of epithelial cells, which, towards the margin or equator, gradually elongate into lens fibres. The whole lens is enclosed in an elastic structureless membrane, and, like the cornea, its transparency is due to the fact that all its constituents have the same refractive index.
The ligament of the lens is the thickened anterior part of the hyaloid membrane which surrounds the vitreous body; it is closely connected to the iris at the ora serrata, and then splits into two layers, of which the anterior is the thicker and blends with the anterior part of the elastic capsule of the lens, so that, when its attachment to the ora serrata is drawn forward by the ciliary muscle, the lens, by its own elasticity, increases its convexity. Between the anterior and posterior splitting of the hyaloid membrane is a circular lymph space surrounding the margin of the lens known as the canal of Petit (fig. 1, p).
The aqueous humour (fig. 1, aq) is contained between the lens and its ligament posteriorly and the cornea anteriorly. It is practically a very weak solution of common salt (chloride of sodium 1.4%). The space containing it is imperfectly divided into a large anterior and a small posterior chamber by a perforated diaphragm—the iris.
The vitreous body or humour is a jelly which fills all the contents of the eyeball behind the lens. It is surrounded by the hyaloid membrane, already noticed, and anteriorly is concave for the reception of the lens.
From the centre of the optic disk to the posterior pole of the lens a lymph canal formed by a tube of the hyaloid membrane stretches through the centre of the vitreous body; this is the canal of Stilling, which in the embryo transmitted the hyaloid artery to the lens. The composition of the vitreous is practically the same as that of the aqueous humour.
The arteries of the eyeball are all derived from the ophthalmic branch of the internal carotid, and consist of the retinal which enters the optic nerve far back in the orbit, the two long ciliaries, which run forward in the choroid and join the anterior ciliaries, from muscular branches of the ophthalmic, in the circulus iridis major round the margin of the iris, and the six to twelve short ciliaries which pierce the sclerotic round the optic nerve and supply the choroid and ciliary processes.
The veins of the eyeball emerge as four or five trunks rather behind the equator; these are called from their appearance venae vorticosae, and open into the superior ophthalmic vein. In addition to these there is a retinal vein which accompanies its artery.
Accessory Structures of the Eye.—The eyelids are composed of the following structures from in front backward: (1) Skin; (2) Superficial fascia; (3) Orbicularis palpebrarum muscle; (4) Tarsal plates of fibrous tissue attached to the orbital margin by the superior and inferior palpebral ligaments, and, at the junction of the eyelids, by the external and internal tarsal ligaments of which the latter is also known as the tendo oculi; (5) Meibomian glands, which are large modified sebaceous glands lubricating the edges of the lids and preventing them adhering, and Glands of Moll, large sweat glands which, when inflamed, cause a “sty”; (6) the conjunctiva, a layer of mucous membrane which lines the back of the eyelids and is reflected on to the front of the globe, the reflection forming the fornix: on the front of the cornea the conjunctiva is continuous with the layer of epithelial cells already mentioned.
The lachrymal gland is found in the upper and outer part of the front of the orbit. It is about the size of an almond and has an upper (orbital) and a lower (palpebral) part. Its six to twelve ducts open on to the superior fornix of the conjunctiva.
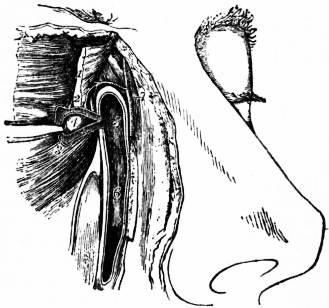
The lachrymal canals (canaliculi) (see fig. 3, 2 and 3) are superior and inferior, and open by minute orifices (puncta) on to the free margins of the two eyelids near their inner point of junction. They collect the tears, secreted by the lachrymal gland, which thus pass right across the front of the eyeball, continually moistening the conjunctiva. The two ducts are bent round a small pink tubercle called the caruncula lachrymalis (fig. 3, 4) at the inner angle of the eyelids, and open into the lachrymal sac (fig. 3, 5), which lies in a groove in the lachrymal bone. The sac is continued down into the nasal duct (fig. 3, 6), which is about ¾ inch long and opens into the inferior meatus of the nose, its opening being guarded by a valve.
 |
|
| Fig. 3.—Lachrymal Canals and Duct. | |
1, Orbicular muscle. 2, Lachrymal canal. 3, Punctum. 4, Caruncula. |
5, Lachrymal sac. 6, Lachrymal duct. 7, Angular artery. |
The orbit contains seven muscles, six of which rise close to the optic foramen. The levator palpebrae superioris is the highest, and passes forward to the superior tarsal plate and fornix of the conjunctiva. The superior and inferior recti are inserted into the upper and lower surfaces of the eyeball respectively; they make the eye look inward as well as up or down. The external and internal recti are inserted into the sides of the eyeball and make it look outward or inward. The superior oblique runs forward to a pulley in the inner and front part of the roof of the orbit, round which it turns to be inserted into the outer and back part of the eyeball. It turns the glance downward and outward. The inferior oblique rises from the inner and front part of the floor of the orbit, and is also inserted into the outer and back part of the eyeball. It directs the glance upward and outward. Of all these muscles the superior oblique is supplied by the fourth cranial nerve, the external rectus by the sixth and the rest by the third.
The posterior part of the eyeball and the anterior parts of the muscles are enveloped in a lymph space, known as the capsule of Tenon, which assists their movements.
 |
 |
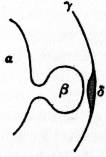
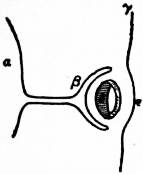
| Fig. 4. Diagram of Developing Eye (1st stage). |
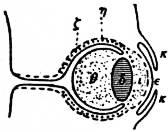
Fig. 5. Diagram of Developing Eye (2nd stage). |
| α, Forebrain. β, Optic vesicle. γ, Superficial ectoderm. δ, Thickening for lens. |
β, Optic cup. δ, Invagination of lens. Other letters as in fig. 4. |
Embryology.—As is pointed out in the article Brain, the optic vesicles grow out from the fore-brain, and the part nearest the brain becomes constricted and elongated to form the optic stalk (see figs. 4 and 5, β). At the same time the ectoderm covering the side of the head thickens and becomes invaginated to form the lens vesicle (see figs. 4 and 5, δ), which later loses its connexion with the surface and approaches the optic vesicle, causing that structure to become cupped for its reception, so that what was the optic vesicle becomes the optic cup and consists of an external and an internal layer of cells (fig. 6 β and δ). Of these the outer cells become the retinal pigment, while the inner form the other layers of the retina. The invagination of the optic cup extends, as the choroidal fissure (not shown in the diagrams), along the lower and back part of the optic stalk, and into this slit sinks some of the surrounding mesoderm to form the vitreous body and the hyaloid arteries, one of which persists.1 When this has happened the fissure closes up. The anterior epithelium of the lens vesicle remains, but from the posterior the lens fibres are developed and these gradually fill up the cavity. The superficial layer of head ectoderm, from which the lens has been invaginated and separated, becomes the anterior epithelium of the cornea (fig. 6, ε), and between it and the lens the mesoderm sinks in to form the cornea, iris and anterior chamber of the eye, while surrounding the optic cup the mesoderm forms the sclerotic and choroid coats (fig. 7, η and ζ). Up to the seventh month the pupil is closed by the membrana pupillaris, derived from the capsule of the lens which is part of the mesodermal ingrowth through the choroidal fissure already mentioned. The hyaloid artery remains, as a prolongation of the retinal artery to the lens, until just before birth, but after that its sheath forms the canal of Stilling. Most of the fibres of the optic nerve are centripetal and begin as the axons of the ganglionic cells of the retina; a few, however, are centrifugal and come from the nerve cells in the brain.
 |
| Fig. 6. |
| Diagram of Developing Eye (3rd stage). |
δ, Solid lens. ε, Corneal epithelium. Other letters as in figs. 4 and 5. |
 |
| Fig. 7. |
| Diagram of Developing Eye (4th stage). The mesodermal tissues are dotted. |
ζ, Choroid and Iris. η, Sclerotic and Cornea. θ, Vitreous. ε, Aqueous. κ, Eyelids. |
The eyelids are developed as ectodermal folds, which blend with one another about the third month and separate again before birth in Man (fig. 7, κ). The lachrymal sac and duct are formed from solid ectodermal thickenings which later become canalized.
It will thus be seen that the optic nerve and retina are formed from the brain ectoderm; the lens, anterior epithelium of the cornea, skin of the eyelids, conjunctiva and lachrymal apparatus from the superficial ectoderm; while the sclerotic, choroid, vitreous and aqueous humours as well as the iris and cornea are derived from the mesoderm.
See Human Embryology, by C.S. Minot (New York); Quain’s Anatomy, vol. i. (1908); “Entwickelung des Auges der Wirbeltiere,” by A. Froriep, in Handbuch der vergleichenden und experimentellen Entwickelungslehre der Wirbeltiere (O. Hertwig, Jena, 1905).
Comparative Anatomy.—The Acrania, as represented by Amphioxus (the lancelet), have a patch of pigment in the fore part of the brain which is regarded as the remains of a degenerated eye. In the Cyclostomata the hag (Myxine) and larval lamprey (Ammocoetes) have ill-developed eyes lying beneath the skin and devoid of lens, iris, cornea and sclerotic as well as eye muscles. In the adult lamprey (Petromyzon) these structures are developed at the metamorphosis, and the skin becomes transparent, rendering sight possible. Ocular muscles are developed, but, unlike most vertebrates, the inferior rectus is supplied by the sixth nerve while all the others are supplied by the third. In all vertebrates the retina consists of a layer of senso-neural cells, the rods and cones, separated from the light by the other layers which together represent the optic ganglia of the invertebrates; in the latter animals, however, the senso-neural cells are nearer the light than the ganglia.
In fishes the eyeball is flattened in front, but the flat cornea is compensated by a spherical lens, which, unlike that of other vertebrates, is adapted for near vision when at rest. The iris in some bony fishes (Teleostei) is not contractile. In the Teleostei, too, there is a process of the choroid which projects into the vitreous chamber and runs forward to the lens; it is known as the processus falciformis, and, besides nourishing the lens, is concerned in accommodation. This specialized group of fishes is also remarkable for the possession of a so-called choroid gland, which is really a rete mirabile (see Arteries) between the choroid and sclerotic. The sclerotic in fishes is usually chondrified and sometimes calcified or ossified. In the retina the rods and cones are about equal in number, and the cones are very large. In the cartilaginous fishes (Elasmobranchs) there is a silvery layer, called the tapetum lucidum, on the retinal surface of the choroid.
In the Amphibia the cornea is more convex than in the fish, but the lens is circular and the sclerotic often chondrified. There is no processus falciformis or tapetum lucidum, but the class is interesting in that it shows the first rudiments of the ciliary muscle, although accommodation is brought about by shifting the lens. In the retina the rods outnumber the cones and these latter are smaller than in any other animals. In some Amphibians coloured oil globules are found in connexion with the cones, and sometimes two cones are joined, forming double or twin cones.
In Reptilia the eye is spherical and its anterior part is often protected by bony plates in the sclerotic (Lacertilia and Chelonia). The ciliary muscle is striated, and in most reptiles accommodation is effected by relaxing the ciliary ligament as in higher vertebrates, though in the snakes (Ophidia) the lens is shifted as it is in the lower forms. Many lizards have a vascular projection of the choroid into the vitreous, foreshadowing the pecten of birds and homologous with the processus falciformis of fishes. In the retina the rods are scarce or absent.
In birds the eye is tubular, especially in nocturnal and raptorial forms: this is due to a lengthening of the ciliary region, which is always protected by bony plates in the sclerotic. The pecten, already mentioned in lizards, is a pleated vascular projection from the optic disk towards the lens which in some cases it reaches. In Apteryx this structure disappears. In the retina the cones outnumber the rods, but are not as numerous as in the reptiles. The ciliary muscle is of the striped variety.
In the Mammalia the eye is largely enclosed in the orbit, and bony plates in the sclerotic are only found in the monotremes. The cornea is convex except in aquatic mammals, in which it is flattened. The lens is biconvex in diurnal mammals, but in nocturnal and aquatic it is spherical. There is no pecten, but the numerous hyaloid arteries which are found in the embryo represent it. The iris usually has a circular pupil, but in some ungulates and kangaroos it is a transverse slit. In the Cetacea this transverse opening is kidney-shaped, the hilum of the kidney being above. In many carnivores, especially nocturnal ones, the slit is vertical, and this form of opening seems adapted to a feeble light, for it is found in the owl, among birds. The tapetum lucidum is found in Ungulata, Cetacea and Carnivora. The ciliary muscle is unstriped. In the retina the rods are more numerous than the cones, while the macula lutea only appears in the Primates in connexion with binocular vision.
Among the accessory structures of the eye the retractor bulbi muscle is found in amphibians, reptiles, birds and many mammals; its nerve supply shows that it is probably a derivative of the external or posterior rectus. The nictitating membrane or third eyelid is well-developed in amphibians, reptiles, birds and some few sharks; it is less marked in mammals, and in Man is only represented by the little plica semilunaris. When functional it is drawn across the eye by special muscles derived from the retractor bulbi, called the bursalis and pyramidalis. In connexion with the nictitating membrane the Harderian gland is developed, while the lachrymal gland secretes fluid for the other eyelids to spread over the conjunctiva. These two glands are specialized parts of a row of glands which in the Urodela (tailed amphibians) are situated along the lower eyelid; the outer or posterior part of this row becomes the lachrymal gland, which in higher vertebrates shifts from the lower to the upper eyelid, while the inner or anterior part becomes the Harderian gland. Below the amphibians glands are not necessary, as the water keeps the eye moist.
The lachrymal duct first appears in the tailed amphibians; in snakes and gecko lizards, however, it opens into the mouth.
For literature up to 1900 see R. Wiedersheim’s Vergleichende Anatomie der Wirbeltiere (Jena, 1902). Later literature is noticed in the catalogue of the Physiological Series of the R. College of Surgeons of England Museum, vol. iii. (London, 1906).
Eye Diseases.—The specially important diseases of the eye are those which temporarily or permanently interfere with sight. In considering the pathology of the eye it may be remembered that (1) it is a double organ, while (2) either eye may have its own trouble.
1. The two eyes act together, under normal conditions, for all practical purposes exactly as if there were but one eye placed in the middle of the face. All impressions made upon either retina, to the one side of a vertical line through the centre, the fovea centralis, before giving rise to conscious perception cause a stimulation of the same area in the brain. Impressions formed simultaneously, for instance, on the right side of the right retina and on corresponding areas of the right side of the left retina, are conveyed to the same spots in the right occipital lobe of the brain. Pathological processes, therefore, which are localized in the right or left occipital lobes, or along any part of the course of the fibres which pass from the right or left optic tracts to these “visual centres,” cause defects in function of the right or left halves of the two retinae. Hemianopia, or half-blindness, arising from these pathological changes, is of very varying degrees of severity, according to the nature and extent of the particular lesion. The blind areas in the two fields of vision, corresponding to the outward projection of the paralysed retinal areas, are always symmetrical both in shape and degree. The central lesion may for instance be very small, but at the same time destructive to the nerve tissue. This will be revealed as a sector-shaped or insular symmetrical complete blindness in the fields of vision to the opposite side. Or a large central area, or an area comprising many or all of the nerve fibres which pass to the visual centre on one side, may be involved in a lesion which causes impairment of function, but no actual destruction of the nerve tissue. There is thus caused a symmetrical weakening of vision (amblyopia) in the opposite fields. In such cases the colour vision is so much more evidently affected than the sense of form that the condition has been called hemiachromatopsia or half-colour blindness. Hemianopia may be caused by haemorrhage, by embolism, by tumour growth which either directly involves the visual nerve elements or affects them by compression and by inflammation. Transitory hemianopia is rare and is no doubt most frequently of toxic origin.
The two eyes also act as if they were one in accommodating. It is impossible for the two eyes to accommodate simultaneously to different extents, so that where there is, as occasionally happens, a difference in focus between them, this difference remains the same for all distances for which they are adapted. In such cases, therefore, both eyes cannot ever be accurately adapted at the same time, though either may be alone. It often happens as a consequence that the one eye is used to receive the sharpest images of distant, and the other of near objects. Any pathological change which leads to an interference in the accommodating power of one eye alone must have its origin in a lesion which lies peripherally to the nucleus of the third cranial nerve. Such a lesion is usually one of the third nerve itself. Consequently, a unilateral accommodation paresis is almost invariably associated with pareses of some of the oculo-motor muscles. A bilateral accommodation paresis is not uncommon. It is due to a nuclear or more central cerebral disturbance. Unlike a hemianopia, which is mostly permanent, a double accommodation paresis is frequently transitory. It is often a post-diphtheritic condition, appearing alone or associated with other paresis.
Both eyes are also normally intimately associated in their movements. They move in response to a stimulus or a combination of stimuli, emanating from different centres of the brain, but one which is always equally distributed to the corresponding muscles in both eyes, so that the two lines of fixation meet at the succession of points on which attention is directed. The movements are thus associated in the same direction, to the right or left, upwards or downwards, &c. In addition, owing to the space which separates the two eyes, convergent movements, caused by stimuli equally distributed between the two internal recti, are required for the fixation of nearer and nearer-lying objects. These movements would not be necessary in the case of a single eye. It would merely have to accommodate. The converging movements of the double eye occur in association with accommodation, and thus a close connexion becomes established between the stimuli to accommodation and convergence. All combinations of convergent and associated movements are constantly taking place normally, just as if a single centrally-placed eye were moved in all directions and altered its accommodation according to the distance, in any direction, of the object which is fixed.
Associated and convergent movements may be interfered with pathologically in different ways. Cerebral lesions may lead to their impairment or complete abolition, or they may give rise to involuntary spasmodic action, as the result of paralysing or irritating the centres from which the various co-ordinated impulses are controlled or emanate. Lesions which do not involve the centres may prevent the response to associated impulses in one eye alone by interfering with the functional activity of one or more of the nerves along which the stimuli are conveyed. Paralysis of oculo-motor nerves is thus a common cause of defects of association in the movements of the double eye. The great advantage of simultaneous binocular vision—viz. the appreciation of depth, or stereoscopic vision—is thus lost for some, or it may be all directions of fixation. Instead of seeing singly with two eyes, there is then double-vision (diplopia). This persists so long as the defect of association continues, or so long as the habit of mentally suppressing the image of the faultily-directed eye is not acquired.
In the absence of any nerve lesions, central or other, interfering with their associated movements, the eyes continue throughout life to respond equally to the stimuli which cause these movements, even when, owing to a visual defect of the one eye, binocular vision has become impossible. It is otherwise, however, with the proper co-ordination of convergent movements. These are primarily regulated by the unconscious desire for binocular vision, and more or less firmly associated with accommodation. When one eye becomes blind, or when binocular vision for other reasons is lost, the impulse is gradually, as it were, unlearnt. This is the cause of divergent concomitant squint. Under somewhat similar conditions a degree of convergence, which is in excess of the requirements of fixation, may be acquired from different causes. This gives rise to convergent concomitant squint.
For Astigmatism, &c., see the article Vision.
2. Taking each eye as a single organ, we find it to be subject to many diseases. In some cases both eyes may be affected in the same way, e.g. where the local disease is a manifestation of some general disturbance. Apart from the fibrous coat of the eye, the sclera, which is little prone to disease, and the external muscles and other adnexa, the eye may be looked upon as composed of two elements, (a) the dioptric media, and (b) the parts more or less directly connected with perception. Pathological conditions affecting either of these elements may interfere with sight.
The dioptric media, or the transparent portions which are concerned in the transmission of light to, and the formation of images upon, the retina, are the following: the cornea, the aqueous humour, the crystalline lens and the vitreous humour. Loss of transparency in any of these media leads to blurring of the retinal images of external objects. In addition to loss of transparency the cornea may have its curvature altered by pathological processes. This necessarily causes imperfection of sight. The crystalline lens, on the other hand, may be dislocated, and thus cause image distortion.
The Cornea.—The transparency of the cornea is mainly lost by imflammation (keratitis), which causes either an infiltration of its tissues with leucocytes, or a more focal, more destructive ulcerative process.
Inflammation of the cornea may be primary or secondary, i.e. the inflammatory changes met with in the corneal tissue may be directly connected with one or more foci of inflammation in the cornea itself or the focus or foci may be in some other part of the eye. Only the very superficial forms of primary keratitis, those confined to the epithelial layer, leave no permanent change; there is otherwise always a loss of tissue resulting from the inflammation and this loss is made up for by more or less densely intransparent connective tissue (nebula, leucoma). These according to their site and extent cause greater or less visual disturbance. Primary keratitis may be ulcerative or non-ulcerative, superficial or deep, diffuse or circumscribed, vascularized or non-vascularized. It may be complicated by deeper inflammations of the eye such as iritis and cyclitis. In some cases the anterior chamber is invaded by pus (hypopyon). The healing of a corneal ulcer is characterized by the disappearance of pain where this has been a symptom and by the rounding off of its sharp margins as epithelium spreads over them from the surrounding healthy parts. Ulcers tend to extend either in depth or superficially, rarely in both manners at the same time. A deep ulcer leads to perforation with more or less serious consequences according to the extent of the perforation. Often an eye bears permanent traces of a perforation in adhesion of the iris to the back of a corneal scar or in changes in the lens capsule (capsular cataract). In other cases the ulcerated cornea may yield to pressure from within, which causes it to bulge forwards (staphyloma).
The principal causes of primary keratitis are traumata and infection from the conjunctiva. Traumata are most serious when the body causing the wound is not aseptic or when micro-organisms from some other source, often the conjunctiva and tear-sac, effect a lodgment before healing of the wound has sufficiently advanced. In infected cases a complication with iritis is not uncommon owing to the penetration of toxines into the anterior chamber.
Inflammations of the cornea are the most important diseases of the eye, because they are among the most frequent, because of the value of the cornea to vision and because much good can often be done by judicious treatment and much harm result from wrong interference and neglect. The treatment of primary keratitis must vary according to the cause. Generally speaking the aim should be to render the ulcerated portions as aseptic as possible without using applications which are apt to cause a great deal of irritation and thus interfere with healing. On this account it is important to be able to recognize when healing is taking place, for as soon as this is the case, rest, along with frequent irrigation of the conjunctiva with sterilized water at the body temperature, and occasionally mild antiseptic irrigation of the nasal mucous membrane is all that is required. It is a common and dangerous mistake to over treat.
Of local antiseptics which are of use may be mentioned the actual cautery, chlorine water, freshly prepared silver nitrate or protargol, and the yellow oxide of mercury. These different agents are of course not all equally applicable in any given case; it depends upon the severity as well as upon the nature of the inflammation which is the most suitable. For instance, the actual cautery is employed only in the case of the deeper septic or malignant ulcers, in which the destruction of tissue is already considerable and tending to spread further. Again the yellow oxide of mercury should only be used in the more superficial, strumous forms of inflammation. Many other substances are also in use, but need not here be referred to.
Secondary keratitis takes the form of an interstitial deposit of leucocytes between the layers of the cornea as well as often of vascularization, sometimes intense, from the deeper network of vessels (anterior ciliary) surrounding the cornea. The duration of a secondary keratitis is usually prolonged, often lasting many months. More or less complete restoration of transparency is the rule, however, eventually.
No local treatment is called for except the shading of the eyes and in most cases the use of a mydriatic to prevent synechiae when the iris is involved. Often it is advisable to do something for the general health. In young people there is probably nothing better than cod-liver oil and syrup of the iodide of iron. Inherited syphilis, tuberculous and other inflammations are the causes of secondary keratitis.
Neuro-paralytic Keratitis.—When the fifth nerve is paralysed there is a tendency for the cornea to become inflamed. Different forms of inflammation may then occur which all, besides anaesthesia, show a marked slowness in healing. The main cause of neuro-paralytic keratitis lies in the greater vulnerability of the cornea. The prognosis is necessarily bad. The treatment consists in as far as possible protecting the eye from external influences, by keeping it tied up, and by frequently irrigating with antiseptic lotions.
Certain non-inflammatory and degenerative changes are met with in the cornea. Of these may be mentioned keratoconus or conical cornea, in which, owing to some disturbance of vitality, the nature of which has not been discovered, the normal curvature of the cornea becomes altered to something more of a hyberboloid of revolution, with consequent impairment of vision: arcus senilis, a whitish opacity due to fatty degeneration, extending round the corneal margin, varying in thickness in different subjects and usually only met with in old people: transverse calcareous film, consisting of a finely punctiform opacity extending, in a tolerably uniformly wide band, occupying the zone of the cornea which is left uncovered when the lids are half closed.
Tumours of the cornea are not common. Those chiefly met with are dermoids, fibromata, sarcomata and epitheliomata.
Scleritis.—Inflammation of the sclera is confined to its anterior part which is covered by conjunctiva. Scleritis may occur in circumscribed patches or may be diffused in the shape of a belt round the cornea. The former is usually more superficial and uncomplicated, the latter deeper and complicated with corneal infiltration, irido-cyclitis and anterior choroiditis. Superficial scleritis or, as it is often called, episcleritis, is a long-continued disease which is associated with very varying degrees of discomfort. The chronic nature of the affection depends mainly upon the tendency that the inflammation has to recur in successive patches at different parts of the sclera. Often only one eye at a time is affected. Each patch lasts for a month or two and is succeeded by another after an interval of varying duration. Months or years may elapse between the attacks. The cicatricial site of a previous patch is rarely again attacked. The scleral infiltration causes a firm swelling, often sensitive to touch, over which the conjunctiva is freely movable. The overlying conjunctiva is always injected. The infiltration itself at the height of the process is densely vascularized. Seen through the conjunctiva its vessels have a darker, more purplish hue than the superficial ones. The swelling caused by the infiltration gradually subsides, leaving a cicatrix to which the overlying conjunctiva becomes adherent. The cicatrix has a slaty porcellanous-looking colour. Superficial scleritis occurs in both sexes with about equal frequency. No definite cause for the inflammation is known. The treatment on the whole is unsatisfactory. Burning down the nodules with the actual cautery, and subsequently a visit to such baths as Harrogate, Buxton, Homburg and Wiesbaden, may be recommended.
Deep scleritis with its attendant complications is altogether a more serious disease. Etiologically it is equally obscure. Both eyes are almost always attacked. It more generally occurs in young people, mostly in young women. Deep scleritis is more persistent and less subject to periods of intermission than episcleritis. The deeper and more wide-spread inflammatory infiltrations of the sclera lead eventually to weakening of that coat, and cause it to yield to the intra-ocular pressure. Vision suffers from extension of the infiltration to the cornea, or from iritis with its attendant synechiae, or from anterior choroiditis, and sometimes also from secondary glaucoma. The treatment is on the whole unsatisfactory. Iridectomy, especially if done early in the process, may be of use.
The Aqueous Humour.—Intransparency of the aqueous humour is always due to some exudation. This comes either from the iris or the ciliary processes, and may be blood, pus or fibrin. An exudation in this situation tends naturally to gravitate to the most dependent part, and, in the case of blood or pus, is known as kyphaema or hypopyon.
The Crystalline Lens Cataract.—Intransparency of the crystalline lens is technically known as cataract. Cataract may be idiopathic and uncomplicated, or traumatic, or secondary to disease in the deeper parts of the eye. The modified epithelial structure of which the lens is composed is always being added to throughout life. The older portions of the lens are consequently the more central. They are harder and less elastic. This arrangement seems to predispose to difficulties of nutrition. In many people, in the absence altogether of general or local disease, the transparency of the lens is lost owing to degeneration of the incompletely-nourished fibres. This idiopathic cataract mostly occurs in old people; hence the term senile cataract. So-called senile cataract is not, however, necessarily associated with any general senile changes. An idiopathic uncomplicated cataract is also met with as a congenital defect due to faulty development of the crystalline lens. A particular and not uncommon form of this kind of cataract, which may also develop during infancy, is lamellar or zonular cataract. This is a partial and stationary form of cataract in which, while the greater part of the lens retains its transparency, some of the lamellae are intransparent. Traumatic cataract occurs in two ways: by laceration or rupture of the lens capsule, or by nutritional changes consequent upon injuries to the deeper structures of the eye. The transparency of the lens is dependent upon the integrity of its capsule. Penetrating wounds of the eye involving the capsule, or rupture of the capsule from severe blows on the eye without perforation of its coats, are followed by rapidly developing cataract. Severe non-penetrating injuries, which do not cause rupture of the capsule, are sometimes followed, after a time, by slowly-progressing cataract. Secondary cataract is due to abnormalities in the nutrient matter supplied to the lens owing to disease of the ciliary body, choroid or retina. In some diseases, as diabetes, the altered general nutrition tells in the same way on the crystalline lens. Cataract is then rapidly formed. All cases of cataract in diabetes are not, however, necessarily true diabetic cataracts in the above sense. Dislocations of the lens are traumatic or congenital. In old-standing disease of the eye the suspensory ligament may yield in part, and thus lead to lens dislocation. The lens is practically always cataractous before this takes place.
The Vitreous Humour.—The vitreous humour loses its transparency owing to exudation from the inflamed ciliary body or choroid. The exudation may be fibrinous or purulent; the latter only as a result of injuries by which foreign bodies or septic matter are introduced into the eye or in metastatic choroiditis. Blood may also be effused into the vitreous from rupture of retinal, ciliary or choroidal vessels. The pathological significance of the various effusions into the vitreous depends greatly upon the cause. In many cases effusion and absorption are constantly taking place simultaneously. The extent of possible clearing depends greatly upon the preponderance of the latter process.
Diseases of the Iris and Ciliary Body.—Inflammation of the iris, iritis, arises from different causes. The various idiopathic forms have relations to constitutional disturbances such as rheumatism, gout, albuminuria, tuberculosis, fevers, syphilis, gonorrhoea and others, or they may come from cold alone. Traumatic and infected cases are attributable to accidents, the presence of foreign bodies, operations, &c. In addition, iritis may be secondary to keratitis, scleritis or choroiditis. The beginning of an attack of inflammation of the iris is characterized by alterations in its colour due to hyperaemia and by circumcorneal injection. Later on, exudation takes place into the substance of the iris, causing thickening and also a loss of gloss of its surface. According to the nature and severity of the exudation there may be deposits formed on the back of the cornea, attachments between the iris and lens capsule (synechiae), or even gelatinous-looking coagulations or pus in the anterior chamber.
The subjective symptoms to which the inflammation may give rise are dread of light (photophobia), pain, generally most severe at night and often very great, also more or less impairment of sight. Along with the pain and photophobia there is lacrymation. An acute attack of iritis usually lasts about six weeks. Some cases become chronic and last much longer. Others are chronic from the first, and in one clinical type of iritis, in which the ciliary body is also at the same time affected, viz. iritis serosa, there is usually comparatively little injection of the eye or pain, so that the patient’s attention may only be directed to the eye owing to the gradual impairment of sight which results. In some cases, and more particularly in men, there is a tendency to the recurrence at longer or shorter intervals of attacks of iritis (recurrent iritis). In these cases, as well as in all cases of plastic iritis which have not been properly treated, serious consequences to sight are apt to follow from the binding down of the iris to the lens capsule and the occlusion of the pupil by exudation.
Inflammation of the ciliary body, cyclitis, is frequently associated with iritis. This association is probable in all cases where there are deposits on the posterior surface of the cornea. It is certain where there are changes in the intra-ocular tension. Often in cyclitis there is a very marked diminution in tension. Cyclitis is also present when the degree of visual disturbance is greater than can be accounted for by the visible changes in the pupil and anterior chamber. The exudation may, as in iritis, be serous, plastic or purulent. It passes from the two free surfaces of the ciliary body into the posterior aqueous, and into the vitreous, chambers. This produces, what is a constant sign of cyclitis, more or less intransparency of the vitreous humour. Where there has been excessive exudation into the vitreous, subsequent shrinking and liquefaction take place, leading to detachment of the retina and consequent blindness.
The treatment of iritis necessarily differs to some extent according to the cause. The general treatment applicable to all cases need only be here considered. What should be aimed at, at the time of the inflammation, is to put the eye as far as possible at rest, to prevent the formation of synechiae and alleviate the pain. An attempt should be made to get the pupil thoroughly dilated with atropine. The dilatation should be kept up as long as any circumcorneal injection lasts. If a case of iritis be left to itself or treated without the use of a mydriatic, posterior synechiae almost invariably form. Some fibrinous exudation may even organize into a membrane stretching across, and more or less completely occluding, the pupil. Synechiae, though not of themselves causing impairment of vision, increase the risk that the eye runs from subsequent attacks of iritis. It should however be remembered that as the main call for a mydriatic is to prevent synechiae, the raison d’être for its use no longer exists when, having been begun too late, the pupil cannot properly be dilated by it. Under these conditions it may even do harm. The eyes should also be kept shaded from the light by the use of a shade or neutral-tinted glasses. During an attack any use of the eyes for reading or sewing or work of any kind calling for accommodation must be prohibited. This applies equally to the case of inflammation in one eye alone and in both.
Pain is best relieved by hot fomentations, cocain, and in many cases the internal use of salicin or phenacetin. The treatment sometimes required for cases of old iritis is iridectomy. The operation is called for in two different classes of cases. In the first place, to improve vision where the pupil is small, and to a great extent occluded, though the condition has not so far led to serious nutritive changes; and in the second place, with the object as well of preventing the complete destruction of vision which either the existing condition or the danger of recurrence of the inflammation has threatened. Iridectomy for iritis should be performed when the inflammation has entirely subsided. The portion of iris excised should be large. The operation is urgently called for where the condition of iris bombans exists.
Iris tumours, either simple or malignant, are of rare occurrence.
A frequent result of a severe blow on the eye is a separation of a portion of the iris from its peripheral attachment (iridodialysis). Of congenital anomalies the most commonly met with are coloboma and more or less persistence of the foetal pupillary membrane. The most serious form of irido-cyclitis is that which may follow penetrating wounds of the eye. Under certain conditions this leads to a similar inflammation in the other eye. This so-called sympathetic ophthalmitis is of a malignant type, causing destruction of the sympathizing eye.
The Retina.—Choroidal inflammations are generally patchy, various foci of inflammation being scattered over the choroid. These patches may in course of time become more or less confluent. The effect upon vision depends upon the extent to which the external or percipient elements of the retina become involved. It is especially serious when the more central portions of the retina, are thus affected (choroido-retinitis centralis).
A peculiar and grave pathological condition of the eye is what is known as glaucoma. A characteristic of this condition is increase of the intra-ocular tension, which has a deleterious effect on the optic nerve end and its ramifications in the retina. The cause of the rise of tension is partly congestive, partly mechanical. The effect of glaucoma, when untreated, is to cause ever-increasing loss of sight, although the time occupied by the process before it leads to complete blindness varies within such extraordinary wide limits as from a few hours to many years. The uveal tract may be the site of sarcoma.
The retina is subject to inflammation, to detachment from the choroid, to haemorrhages from the blood-vessels and to tumour. Retinal inflammation may primarily affect either the nerve elements or the connective tissue framework. The former is usually associated with some general disease such as albuminuria or diabetes and is bilateral. The tissue changes are oedema, the formation of exudative patches, and haemorrhage. Where the connective tissue elements are primarily affected, the condition is a slow one, similar to sclerosis of the central nervous system. The gradual blindness which this causes is due to compression of the retinal nerve elements by the connective tissue hyperplasia, which is always associated with characteristic changes in the disposition of the retinal pigment. This retinal sclerosis is consequently generally known as retinitis pigmentosa, a disease to which there is a hereditary predisposition. Besides occurring during inflammation, haemorrhages into the retina are met with in phlebitis of the central retinal vein, which is almost invariably unilateral, and in certain conditions of the blood, as pernicious anaemia, when they are always bilateral.
The optic nerve is subject to inflammation (optic neuritis) and atrophy. Double optic neuritis, affecting, however, only the intra-ocular ends of the nerves, is an almost constant accompaniment of brain tumour. Unilateral neuritis has a different causation, depending upon an inflammation, mainly perineuritic, of the nerve in the orbit. It is analogous to peripheral inflammation of other nerves, such as the third, fourth, sixth and seventh cranial nerves.
Diseases of the Conjunctiva.—These are the most frequent diseases of the eye with which the surgeon has to deal. They generally lead to more or less interference with the functional activity of the eye and often indeed to great impairment of vision owing to the tendency which there is for the cornea to become implicated.
Many different micro-organisms are of pathogenetic importance in connexion with the conjunctiva. Microbes exist in the normal conjunctival sac. These are mostly harmless, though it is usual to find at any rate a small proportion of others which are known to be pyogenetic. This fact is of great importance in connexion both with problems of etiology and the practical question of operations on the eye.
Hyperaemia.—When the conjunctiva becomes hyperaemic its colour is heightened and its transparency lessened. Sometimes too it becomes thickened and its surface altered in appearance. The often marked heightening of colour is due to the very superficial position of the dilated vessels. This is specially the case with that part of the membrane which forms the transition fold between the palpebral and the ocular conjunctiva. Consequently it is there that the redness is most marked, while it is seen to diminish towards the cornea. An important diagnostic mark is thus furnished between purely conjunctival hyperaemia and what is called circumcorneal congestion, which is always an indication of more deep-seated vascular dilatation. It also differs materially from a scleral injection, in which there is a visible dilatation of the superficial scleral vessels.
When a conjunctival hyperaemia has existed for some time the papillae become swollen, and small blebs form on the surface of the membrane: sometimes too, lymph follicles begin to show. The enlargement and compression of adjacent papillae give rise to a velvety appearance of the surface.
Hyperaemia of the conjunctiva where not followed by inflammation causes more or less lacrymation but no alteration in the character of its secretion. The hyperaemia may be acute and transitory or chronic. Much depends upon the cause as well as upon the persistence of the irritation which sets it up.
Traumata, the presence of foreign bodies in the conjunctival sac, or the irritations of superficial chalky infarcts in the Meibomian ducts, cause more or less severe transitory congestion. Continued subjection to irritating particles such as flour, stones, dust, &c. , causes a more continued hyperaemia which is often circumscribed and less pronounced. Bad air in schools, barracks, workhouses, &c. , also causes a chronic hyperaemia in which it is common to find a follicular hyperplasia. Long exposure to too intense light, astigmatism and other ocular defects which cause asthenopia lead also to chronic hyperaemia. Anaemic individuals are often subject to discomfort from hyperaemia of this nature.
The treatment of conjunctival hyperaemia consists first in the removal of the cause when it can be discovered. Often this is difficult. In addition the application of hot sterilized water is useful and soothing.
Conjunctivitis.—When the conjunctiva is actually inflamed the congested membrane is brought into a condition of heightened secreting action. The secretions become more copious and more or less altered in character. A sufficiently practical though by no means sharply defined clinical division of cases of conjunctivitis is arrived at by taking into consideration the character of the secretion from the inflamed membrane and the visible tissue alterations which the membrane undergoes. The common varieties of conjunctivitis which may thus be distinguished are the following: (α) Catarrhal conjunctivitis, (β) Purulent conjunctivitis, (γ) Phlyctenular conjunctivitis, (δ) Granular conjunctivitis and (ε) Diphtheritic conjunctivitis.
However desirable a truly etiological classification might appear to be, it is doubtful whether such could satisfactorily be made. So much is certain at all events, that not only can identically the same clinical appearance result from the actions of quite different pathogenetic organisms, but that various concomitant circumstances may lead to very different clinical signs being set up by one and the same microbe. As regards contagion there is no doubt that the secretion in the case of a true conjunctivitis (i.e. not merely a hyperaemia) is always more or less contagious. The degree of virulence varies not only in different cases, but the effect of contagion from the same source may be different in different individuals. Healthy conjunctivae may thus react differently, not only as regards the degree of severity, but even according to different clinical types, when infected by secretion from the same source. There are no doubt different reasons for this, such as the stage at which the inflammation has arrived in the eye from which the secretion is derived, differences in the surroundings and in the susceptibility of the infected individuals, the presence of dormant microbes of a virulent type in the healthy conjunctiva which has been infected, &c. Many points in this connexion are very difficult to investigate and much remains to be elucidated. Contagion usually takes place directly and not through the air. Often in this way one eye is first affected and may in some cases, when sufficient care is afterwards taken, be the only one to suffer.
The treatment in all severer forms of conjunctivitis should be undertaken with the primary object in view of preventing any implication of the cornea.
Catarrhal conjunctivitis, which is characterized by an increased mucoid secretion accompanying the hyperaemia, is usually bilateral and may be either acute or chronic. Acute conjunctivitis lasts as a rule only for a week or two: the chronic type may persist, with or without occasional exacerbations, for years. The subjective symptoms vary in intensity with the severity of the inflammation. There is always more or less troublesome “burning” in the eyes with a tired heavy feeling in the lids. This is aggravated by reading, which is most distressing in a close or smoky atmosphere and by artificial light. In acute cases, indeed, reading is altogether impossible. In all cases of catarrhal conjunctivitis the symptoms are also more marked if the eyes have been tied up, even though this may produce a temporary relief.
A curious variety of acute catarrhal conjunctivitis, in which the hyperaemia and lacrymation are the predominant features, is the so-called hay-fever. In this condition the mucous membrane of the nose and throat are similarly affected, and there is at the same time more or less constitutional disturbance. Hay-fever is due to irritation from the pollen of many plants, but principally from that of the different grasses. Some people are so susceptible to it that they invariably suffer every year during the early summer months. Here it is difficult to remove the cause, but many cases can be cured and almost all are alleviated be means of a special antitoxin applied locally.
Other ectogenetic causes of catarrhal conjunctivitis which have been studied are mostly microbic. Of these the most common are the Morax-Axenfeld and the Koch-Weeks conjunctivitis.
The Morax-Axenfeld bacillus sets up a conjunctivitis which affects individuals of all ages and conditions and which is contagious. The inflammation is usually chronic, at most subacute. It is often sufficiently characteristic to be recognized without a microscopical examination of the secretions. In typical cases the lid margin, palpebral conjunctiva, and it may be a patch of ocular conjunctiva at the outer or inner angle are alone hyperaemic: the secretion is not copious and is mostly found as a greyish coagulum lying at the inner lid-margin. The subjective symptoms are usually slight. Complications with other varieties of catarrhal conjunctivitis are not uncommon. This mild form of conjunctivitis generally lasts for many months, subject to more or less complete disappearance followed by recurrences. It can be rapidly cured by the use of an oxide of zinc ointment, which should be continued for some time after the appearances have altogether passed off.
The conjunctivitis caused by the Koch-Weeks microbe is still more common. It is a more acute type, affects mostly children, and is very contagious and often epidemic. Here the hyperaemia involves both the ocular and the palpebral conjunctiva, and usually there is considerable swelling of the lids and a copious secretion. Both eyes are always affected. Occasionally the engorged conjunctival vessels give way, causing numerous small extravasations (ecchymoses). Complications with phlyctenulae (vide infra) are common in children. The acute symptoms last for a week or ten days, after which the course is more chronic. Treatment with nitrate of silver in solution is generally satisfactory. Other less frequent microbic causes of catarrhal conjunctivitis yield to the same treatment.
A form of epidemic muco-purulent conjunctivitis is not uncommon, in which the swelling of the conjunctival folds and lids is much more marked and the secretions copious. It is less amenable to treatment and also apt to be complicated by corneal ulceration. The microbe which gives rise to this condition has not been definitely established. This inflammation is also known as school ophthalmia. This is extremely contagious, so that isolation of cases becomes necessary. The treatment with weak solutions of sub-acetate of lead during the acute stage, provided there be no corneal complication, and subsequently with a weak solution of tannic acid, may be recommended.
Purulent Conjunctivitis.—Some of the severer forms of catarrhal conjunctivitis are accompanied not only by a good deal of swelling of both conjunctiva and lids but also by a decidedly muco-purulent secretion. Nevertheless there is a sufficiently sharply-defined clinical difference between the catarrhal and purulent types of inflammation. In purulent conjunctivitis the oedema of the lids is always marked, often excessive, the hyperaemia of the whole conjunctiva is intense: the membrane is also infiltrated and swollen (chemosis), the papillae enlarged and the secretion almost wholly purulent. Although this variety of conjunctivitis is principally due to infection by gonococci, other microbes, which more frequently set up a catarrhal type, may lead to the purulent form.
All forms are contagious, and transference of the secretion to other eyes usually sets up the same type of severe inflammation. The way in which infection mostly takes place is by direct transference by means of the hands, towels, &c. , of secretions containing gonococci either from the eye or from some other mucous membrane. The poison may also sometimes be carried by flies. The dried secretion loses its virulence.
In new-born children (ophthalmia neonatorum) infection takes place from the maternal passages during birth. Notwithstanding the great changes which occur during the progress of a purulent conjunctivitis, there is on recovery a complete restitutio ad integrum so far as the conjunctiva is concerned. Owing to the tendency to severe ulceration of the cornea, more or less serious destructions of that membrane, and consequently more or less interference with sight, may result before the inflammation has passed off. This is a special danger in the case of adults. For this reason when only one eye is affected the first point to be attended to in the treatment is to secure the second eye from contagion by efficient occlusion. The appliance known as Buller’s shield, a watch-glass strapped down by plaster, is the best for this purpose. It not only admits of the patient seeing with the sound eye, but allows the other to remain under direct observation. The treatment otherwise consists in frequent removal of the secretions from the affected eye, and the use of nitrate of silver solution as a bactericide applied directly to the conjunctival surface; sometimes it is necessary to cut away the chemotic conjunctiva immediately surrounding the cornea. When the cornea has become affected efforts may be made with the thermo-cautery or otherwise to limit the area of destruction and thus admit of something being done to improve the vision after all inflammation has subsided. The greatest cleanliness as well as proper antiseptic precautions should of course be observed by every one in any way connected with the treatment of such cases.
Phlyctenular conjunctivitis is an acute inflammation of the ocular conjunctiva, in which little blebs or phlyctenules form, more particularly in the vicinity of the corneal margin, as well as on the epithelial continuation of the conjunctiva which covers the cornea. The inflammation is characterized by being distributed in little circumscribed foci and not diffused as in all other forms of conjunctivitis. In it the conjunctival secretion is not altered, unless there should exist at the same time a complication with some other form of conjunctivitis. This condition is most frequent in children, particularly such as are ill-nourished or are recovering from some illness, e.g. measles. The susceptibility occurs in fact mainly where there exists what used to be called a “strumous” diathesis. In many cases, therefore, there is some kind of tubercular basis for the manifestations. This basis has to do with the susceptibility only, at all events to begin with. The local changes are not tuberculous; their exact origin has not been clearly established. They are in all probability produced by staphylococci.
Many children suffering from phlyctenular conjunctivitis get after a short time an eczematous excoriation of the skin of the nostrils. This excoriated, scabby area contains crowds of staphylococci which find a nidus here, where the copious tear-flow down the nostrils has excoriated and irritated the skin. Lacrymation is indeed a very common concomitant of phlyctenular conjunctivitis. Another frequently distressing symptom is a pronounced dread of light (photophobia), which often leads to convulsive and very persistent closing of the lids (blepharospasm). Indeed the relief of the photophobia is often the most important point to be considered in the treatment of phlyctenular conjunctivitis. The photophobia may be very severe when the local changes are slight. The eyes should be shaded but not bandaged. Cocain may be freely used. The best local application is the yellow oxide of mercury used as an ointment.
Phlyctenular conjunctivitis, and the corneal complications with which it is so often associated, constitute a large proportion (from ¼ to 1⁄3) of all eye affections with which the surgeon has to deal.
Granular Conjunctivitis.—This disease, which also goes by the name of trachoma, is characterized by an inflammatory infiltration of the adenoid tissue of the conjunctiva. The inflammation is accompanied by the formation of so-called granules, and at the same time by a hyperplasia of the papillae. The changes further lead in the course of time to cicatricial transformations, so that a gradual and progressive atrophy of the conjunctiva results. The disease takes its origin most frequently in the conjunctival fold of the upper lid, but eventually as a rule involves the corna and the deeper tissues of the lid, particularly the tarsus.
The etiology of trachoma is unknown. Though a perfectly distinctive affection when fully established, the differential diagnosis from other forms of conjunctivitis, particularly those associated with much follicular enlargement or which have begun as purulent inflammation, may be difficult. Trachoma is mostly chronic. When occurring in an acute form it is more amenable to treatment and less likely to end in cicatricial changes. Fully half the cases of trachoma which occur are complicated by pannus, which is the name given to the affection when it has spread to the cornea. Pannus is a superficial vascularized infiltration of the cornea. The veiling which it produces causes more or less defect of sight.
Various methods of treatment are in use for trachoma. Expression by means of roller-forceps or repeated grattage are amongst the more effective means of surgical treatment, while local applications of copper sulphate or of alum are certainly useful in suitable cases.
Diphtheritic conjunctivitis is characterized by an infiltration into the conjunctival tissues which, owing to great coagulability, rapidly interferes with the nutrition of the invaded area and thus leads to necrosis of the diphtheritic membrane. Conjunctival diphtheria may or may not be associated with diphtheria of the throat. It is essentially a disease of early childhood, not more than 10% of all cases occurring after the age of four. The cornea is exposed to great risk, more particularly during the first few days, and may be lost by necrosis. Subsequent ulceration is not uncommon, but may often be arrested before complete destruction has taken place. The disease is generally confined to one eye, and complicated by swelling of the preauricular glands of that side. It may prove fatal. In true conjunctival diphtheria the exciting cause is the Klebs-Löffler bacillus. The inflammation occurs in very varying degrees of severity. The secretion is at first thin and scant, afterwards purulent and more copious. In severe cases there is great chemosis with much tense swelling of the lids, which are often of an ashy-grey colour. A streptococcus infection produces somewhat similar and often quite as disastrous results.
The treatment must be both general with antitoxin and local with antiseptics. Of rarer forms of conjunctivitis may be mentioned Parinaud’s conjunctivitis and the so-called spring catarrh.
Non-inflammatory Conjunctival Affections.—These are of less importance than conjunctivitis, either on account of their comparative infrequency or because of their harmlessness. The following conditions may be shortly referred to.
Amyloid degeneration, in which waxy-looking masses grow from the palpebral conjunctiva of both lids, often attaining very considerable dimensions. The condition is not uncommon in China and elsewhere in the East.
Essential Shrinking of the Conjunctiva.—This is the result of pemphigus, in which the disease has attacked the conjunctiva and led to its atrophy.
Pterygium is a hypertrophic thickening of the conjunctiva of triangular shape firmly attached by its apex to the superficial layers of the cornea. It is a common condition in warm climates owing to exposure to sun and dust, and often calls for operative interference.
Tumours of the Conjunctiva.—These may be malignant or benign, also syphilitic and tubercular.
1 Some embryologists regard the vitreous body as formed from the ectoderm (see Quain’s Anatomy, vol. i., 1908).